
Hyperbaric oxygen therapy (HBOT) is defined as a medical treatment that delivers 100% pure oxygen at pressures greater than normal atmospheric levels to raise dissolved oxygen in the bloodstream and tissues. In the context of cancer care, HBOT functions as an adjunct therapy, not a standalone cure. It supports conventional treatments by improving tissue oxygenation, enhancing the effectiveness of radiotherapy and chemotherapy, and managing the damaging side effects of radiation. Understanding how HBOT supports cancer treatment gives you a clearer picture of what this therapy can and cannot do, and whether it may be right for your recovery plan.
How does HBOT biologically support cancer treatment?
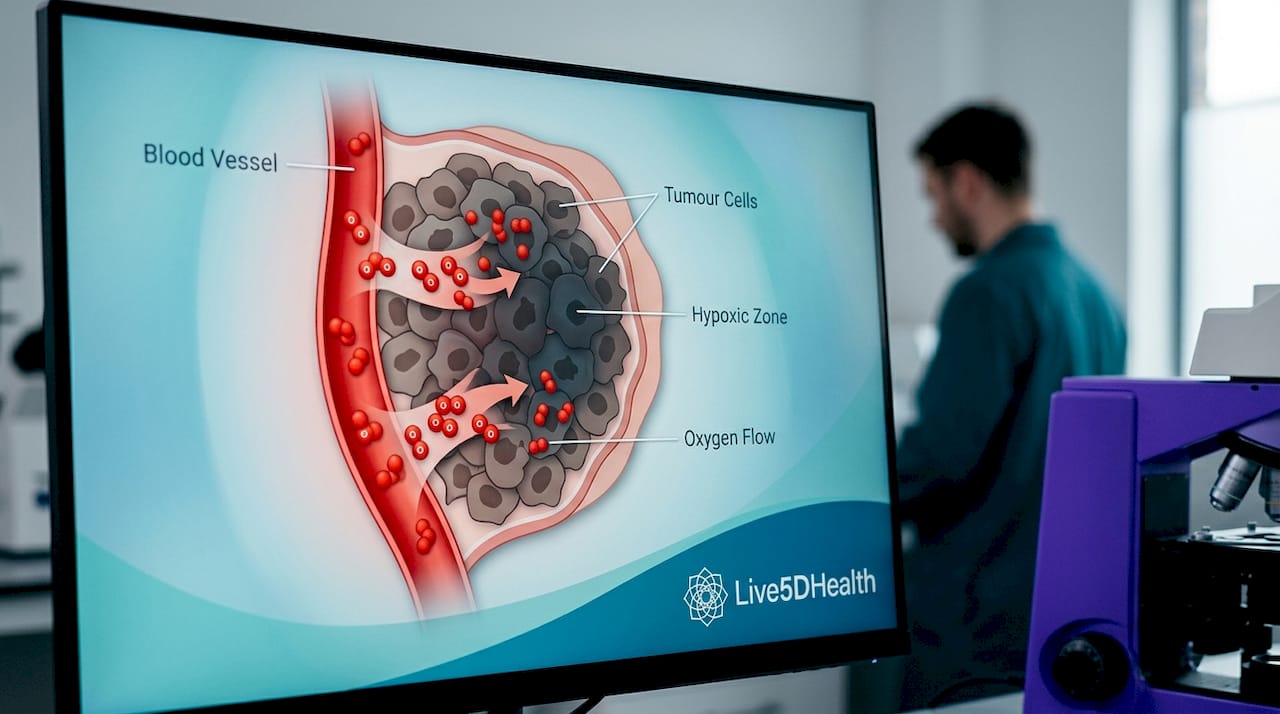
Tumour hypoxia is the central problem that HBOT addresses. Solid tumours frequently develop oxygen-poor zones because their blood supply is disorganised and insufficient. This low-oxygen environment makes cancer cells significantly more resistant to both radiotherapy and chemotherapy, as both treatments rely on oxygen to generate the free radicals that destroy cancer cells.
HBOT works by raising dissolved plasma oxygen to levels that can penetrate these hypoxic zones, effectively reoxygenating tissues that conventional circulation cannot reach. This reoxygenation increases the radiosensitivity of tumour cells, meaning radiation therapy can do more damage to them with the same dose. The same mechanism also augments the cytotoxic effects of certain chemotherapy agents.
Beyond tumour targeting, HBOT promotes angiogenesis (the formation of new blood vessels), collagen synthesis, and tissue repair in areas damaged by radiation. These effects are particularly valuable for patients dealing with late radiation injuries, where normal tissue has been permanently scarred and its blood supply compromised. The therapy also modulates oxidative stress pathways and the tumour microenvironment, which researchers are now investigating in relation to immunotherapy responses.
Key biological effects of HBOT relevant to oncology include:
- Reoxygenation of hypoxic tumour zones, increasing therapy sensitivity
- Stimulation of angiogenesis, supporting healing in radiation-damaged tissue
- Collagen formation and fibroblast activation, aiding structural tissue repair
- Modulation of oxidative stress and ferroptosis pathways, with potential implications for immunotherapy
- Remodelling of the tumour microenvironment, an area of active clinical research
Pro Tip: If you are currently undergoing radiotherapy, ask your oncologist specifically about tumour hypoxia and whether HBOT referral is appropriate for your cancer type and stage. Not all tumours respond equally.
What evidence supports HBOT for managing radiation therapy side effects?
The strongest clinical evidence for HBOT in oncology sits firmly in the management of late radiation toxicities, particularly those affecting the pelvis. Pelvic radiation cystitis and proctitis are two of the most debilitating long-term side effects of radiotherapy for prostate, cervical, bladder, and rectal cancers.
A 2026 systematic review of 42 studies covering 2,785 patients reported response rates of 67 to 100% in pelvic radiation toxicity, with typical HBOT protocols running approximately 34.5 sessions at 2.45 atmospheres absolute (atm). That response range is wide, but even the lower bound represents meaningful relief for patients who have exhausted other options. For radiation proctitis specifically, symptom relief in approximately 89% of patients has been reported, with benefits lasting 6 to 12 months post-treatment.
The picture is less clear for breast and head-and-neck cancers. Randomised trials in these areas have produced inconsistent results, and the Oncology Nursing Society notes that evidence varies considerably by condition and cancer site. HBOT showed reduced pain (32% versus 75%) and reduced fibrosis (33% versus 51%) in certain trials, but these findings have not been uniformly replicated.
“The evidence aligns mechanistic rationale with observed healing of damaged tissues rather than tumour cure. HBOT’s strongest role is supportive management of late radiation toxicities.”
— Supportive Care in Cancer, 2026
| Condition | Evidence level | Typical response |
|---|---|---|
| Pelvic radiation proctitis | Strong (systematic review data) | ~89% symptom relief |
| Pelvic radiation cystitis | Strong (multiple trials) | 67–100% response rate |
| Radiation fibrosis (breast) | Moderate (inconsistent trials) | Reduced fibrosis in some studies |
| Head-and-neck radiation injury | Weak (limited randomised data) | Inconsistent benefit reported |
Safety is generally favourable. The FDA approves HBOT for severe radiation tissue injury as one of its limited indications, and complications are uncommon. The most frequently reported adverse events include ear and sinus barotrauma and transient vision changes, both of which are typically mild and reversible.
What are the practical considerations for HBOT in cancer care?
HBOT is indicated primarily for late radiation tissue injuries rather than as a direct cancer suppression tool. This distinction matters enormously for setting realistic expectations. You are not using HBOT to shrink a tumour. You are using it to heal the tissue damage that radiation has left behind, and to give your body the oxygen environment it needs to recover.
Patient selection follows these general criteria:
- Confirmed late radiation tissue injury such as proctitis, cystitis, osteoradionecrosis, or soft tissue radionecrosis
- Failure or inadequacy of conventional treatments for the radiation injury in question
- Absence of contraindications, including untreated pneumothorax, certain chemotherapy agents (bleomycin, doxorubicin, cisplatin require careful evaluation), and severe chronic obstructive pulmonary disease
- Ability to commit to a full treatment course, typically 30 to 40 sessions over six to eight weeks
- Referral from an oncologist or specialist, with multidisciplinary team input on timing relative to active treatment
Access presents a real challenge. Structural barriers including equipment availability, financial costs, session time commitment, and geographic location of specialised treatment centres limit real-world utilisation. This is why early referral matters. Waiting until symptoms become severe reduces the window for effective intervention.
Adherence to the full course is not optional. Incomplete therapy may fail to achieve the vascular remodelling needed for durable symptom relief, as treatment effects are cumulative and build session by session. Missing sessions or stopping early significantly reduces the likelihood of lasting benefit.
Pro Tip: Ask for a referral to an HBOT centre as soon as radiation-related tissue symptoms appear, rather than waiting to see if they resolve on their own. Early intervention consistently produces better outcomes.
How does HBOT compare with other supportive therapies for radiation damage?
HBOT is not the only option for managing radiation-induced tissue injury, and understanding where it sits relative to alternatives helps you and your care team make informed decisions.
For radiation proctitis, common alternatives include sucralfate enemas, formalin instillation, argon plasma coagulation (endoscopic), and anti-inflammatory agents. For radiation cystitis, bladder irrigation, sodium hyaluronate instillation, and hyperbaric therapy are all used. The table below summarises the main approaches.
| Therapy | Best suited for | Key limitation |
|---|---|---|
| HBOT | Pelvic radiation toxicity, osteoradionecrosis | Requires specialised facility, 30–40 sessions |
| Argon plasma coagulation | Bleeding radiation proctitis | Procedural risk, does not address underlying hypoxia |
| Sucralfate enemas | Mild radiation proctitis | Limited evidence for severe cases |
| Sodium hyaluronate | Radiation cystitis | Short-term symptom relief only |
| Antioxidant supplementation | Radiation fibrosis prevention | Inconsistent clinical evidence |
HBOT’s advantage over most of these alternatives is that it addresses the underlying cause of radiation injury, which is tissue hypoxia and vascular insufficiency, rather than managing surface symptoms. Argon plasma coagulation, for example, stops bleeding but does not restore the oxygen supply that damaged tissue needs to regenerate. This mechanistic depth is why HBOT tends to produce more durable results in well-selected patients.
Combined approaches are increasingly used in practice. HBOT alongside endoscopic intervention, for instance, can address both acute bleeding and the underlying tissue environment. The tumour microenvironment modulation that HBOT provides also makes it a candidate for combination with immunotherapy, though this remains an area of active investigation rather than established practice.
What future research is shaping HBOT’s role in oncology?
The field is moving towards precision dosing and biomarker-driven patient selection, which should resolve some of the inconsistency seen in current trial data. Several directions are particularly worth watching:
- Combination with immunotherapy: HBOT’s ability to remodel the tumour microenvironment and modulate immune pathways makes it a logical partner for checkpoint inhibitors, and early-phase trials are underway
- Optimised protocols: Current standard protocols (approximately 34.5 sessions at 2.45 atm) were developed empirically. Researchers are now investigating whether shorter, higher-pressure protocols or biomarker-guided dosing can improve outcomes
- Chemotherapy combinations: The complex interactions between HBOT and oxidative stress pathways may enhance certain chemotherapy agents, but pro-angiogenic effects raise questions that require careful study
- Long-term safety data: Most current evidence covers outcomes up to 12 months post-treatment. Longer follow-up studies are needed to confirm durability and identify any late adverse effects
- Expanded indications: Osteoradionecrosis of the jaw and soft tissue radionecrosis are areas where HBOT already shows strong mechanistic rationale, and prospective trials are building the evidence base
The honest assessment is that HBOT in oncology is a therapy with a strong mechanistic foundation and good evidence in specific indications, but with significant gaps that well-designed prospective trials must fill. Participating in a clinical trial, if you are eligible, is one of the most meaningful contributions you can make to advancing this field.
Key takeaways
HBOT supports cancer treatment most effectively as an adjunct therapy for late radiation tissue injuries, with the strongest evidence in pelvic toxicities and the greatest uncertainty in breast and head-and-neck cancers.
| Point | Details |
|---|---|
| Primary role is supportive | HBOT manages radiation-induced tissue damage, not the cancer itself. |
| Strongest evidence in pelvic injury | Response rates of 67–100% reported for pelvic radiation proctitis and cystitis. |
| Full course adherence is critical | 30–40 sessions are typically required; incomplete treatment reduces durable benefit. |
| Patient selection determines outcomes | Benefits vary by cancer site, injury type, and prior treatment history. |
| Future research is expanding scope | Combination with immunotherapy and precision dosing protocols are active research areas. |
Why I think HBOT deserves more attention in cancer recovery
Most conversations about cancer treatment focus almost entirely on the primary therapies: surgery, chemotherapy, radiotherapy. What gets far less attention is the quality of life that patients are left with after those treatments end. Radiation-induced proctitis, cystitis, and fibrosis are not minor inconveniences. They are life-altering conditions that can persist for years, and for many patients, they represent the most disruptive part of the entire cancer experience.
What I find genuinely compelling about HBOT is that it addresses the root cause of these injuries rather than papering over the symptoms. When you restore oxygen to tissue that has been starved of it, you give the body a real chance to rebuild. That is not a small thing.
That said, I am cautious about the enthusiasm that sometimes surrounds HBOT in wellness circles. It is not a cancer cure. It does not replace oncology. The evidence for certain cancer types and conditions remains genuinely mixed, and I think it does patients a disservice to overstate what the therapy can achieve. The right approach is to treat HBOT as a powerful tool in a broader recovery plan, one that works best when it is selected carefully, administered consistently, and supported by a multidisciplinary team.
If you are navigating radiation side effects and feel like you have run out of options, HBOT may be exactly what you need. But go in with clear expectations, commit to the full course, and work with clinicians who understand both the promise and the limits of this therapy. You can also explore common HBOT misconceptions before your first consultation, as separating fact from hype will serve you well throughout the process.
— Mark
Discover HBOT and wellness therapies at Live5dhealth
If you are exploring supportive therapies to complement your cancer treatment or recovery, Live5dhealth in Boyle, County Roscommon, offers access to hyperbaric oxygen therapy alongside a full suite of wellness treatments in a luxury retreat setting.
At Live5dhealth, HBOT sessions are structured to align with clinically informed protocols, and the team can discuss how hyperbaric therapy fits alongside other recovery-focused treatments. For those interested in combining therapies, the HBOT and vibro plate combination offers a complementary approach to supporting tissue recovery and overall wellbeing. Whether you are in active recovery or building long-term resilience, Live5dhealth provides a supportive environment designed around your health goals. Visit Live5dhealth HBOT Ireland to learn more about available sessions and next steps.
FAQ
What does HBOT actually do for cancer patients?
HBOT delivers pure oxygen under increased pressure to reoxygenate tissues damaged by radiation, improving healing and reducing symptoms such as pain, bleeding, and fibrosis. It is used as a supportive therapy alongside conventional cancer treatment, not as a replacement for it.
Is HBOT safe during or after cancer treatment?
HBOT is FDA-approved for radiation tissue injury and has a generally favourable safety profile, with mild adverse events such as ear barotrauma and temporary vision changes being the most common. Certain chemotherapy agents and lung conditions require careful evaluation before starting HBOT.
How many HBOT sessions are needed for radiation side effects?
Typical protocols for radiation proctitis and cystitis involve 30 to 40 sessions at approximately 2.45 atm, with each session lasting around 90 minutes. Completing the full course is critical, as the therapeutic effects are cumulative.
Can HBOT help with all types of radiation injury?
Evidence is strongest for pelvic radiation toxicities, including proctitis and cystitis, with response rates of 67 to 100% reported. Results for breast and head-and-neck radiation injuries are more inconsistent, making patient selection and specialist referral particularly important.
Where can I access HBOT in Ireland?
Live5dhealth in Boyle, County Roscommon, offers hyperbaric oxygen therapy as part of its wellness and recovery services. Specialist HBOT centres are also available in larger Irish cities, though geographic access and session commitment remain practical considerations for many patients.