
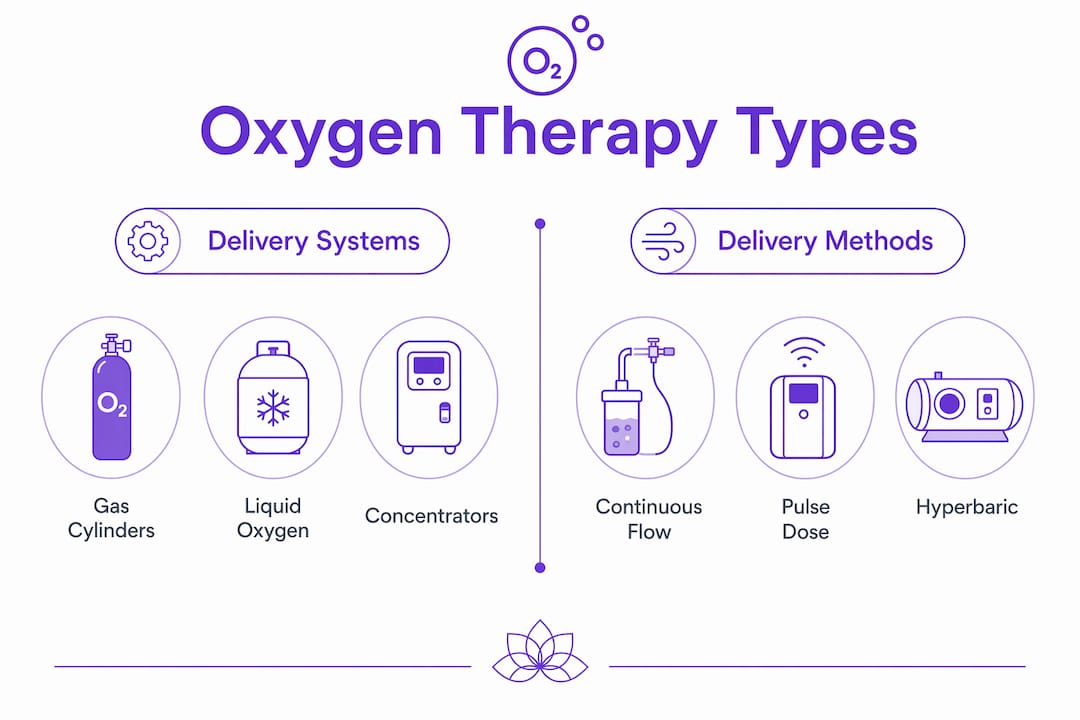
Oxygen therapy is defined as the clinical supplementation of inhaled oxygen beyond ambient air levels to correct or prevent hypoxia, and understanding how oxygen therapy differs by type is the key to choosing the right treatment. The three primary delivery systems are compressed gas cylinders, liquid oxygen, and oxygen concentrators, each operating on a different physical principle. Beyond the storage system, types diverge further by delivery method (continuous flow versus pulse dose), by interface (nasal cannula, Venturi mask, non-rebreather mask), and by therapeutic modality, with hyperbaric oxygen therapy (HBOT) representing an entirely separate category. Whether you are managing a condition like COPD, recovering from an injury, or exploring wellness applications, knowing these differences helps you make confident, informed decisions.
How oxygen therapy differs by type: the main delivery systems
Supplemental oxygen therapy is delivered via three core systems: compressed gas cylinders, liquid oxygen, and oxygen concentrators. Each stores and supplies oxygen differently, which directly affects portability, running costs, and clinical suitability.
| Delivery system | How it works | Best suited for |
|---|---|---|
| Compressed gas cylinders | Pressurised 100% oxygen in metal tanks with a flow regulator | Short-term use, backup supply, emergency settings |
| Liquid oxygen | Cryogenic storage converted to gas on demand; smaller, lighter tanks | Active users needing portability with high purity |
| Stationary concentrator | Extracts oxygen from room air continuously via molecular sieve | Long-term home use with reliable power supply |
| Portable concentrator | Compact concentrator for travel and daily activity | Active patients needing mobility and independence |
Compressed gas cylinders store oxygen at very high pressure, typically above 2,000 psi, in steel or aluminium tanks. They are reliable and deliver 100% pure oxygen, but they are heavy, require regular refilling, and carry pressure-related safety considerations. Hospitals and emergency services depend on them, but for long-term home use they are rarely the first choice.

Liquid oxygen systems store oxygen at extremely low temperatures, around minus 183°C, and convert it to breathable gas on demand. The tanks are significantly smaller and lighter than compressed gas equivalents for the same oxygen volume, making them genuinely practical for people who need portability without sacrificing oxygen purity. The trade-off is that liquid oxygen evaporates over time even when unused, so it suits people who use their system regularly.
Oxygen concentrators extract oxygen directly from ambient air using a zeolite molecular sieve, producing a continuous supply without refilling. Portable concentrators enhance mobility and have transformed quality of life for long-term users. Stationary models are heavier but can run indefinitely from a mains power source, making them the standard choice for home oxygen therapy.
Pro Tip: If you are prescribed home oxygen therapy, ask your clinician whether a portable concentrator with pulse dose delivery would cover your daytime needs, as this combination typically offers the lightest, most travel-friendly setup available.
How do continuous flow and pulse dose oxygen delivery differ?
The delivery method determines when and how oxygen reaches you, and the distinction between continuous flow and pulse dose is one of the most clinically significant oxygen therapy differences you will encounter.
Continuous flow delivers a steady, uninterrupted stream of oxygen at a set number of litres per minute, regardless of whether you are inhaling or exhaling. This means oxygen flows during both phases of the breath cycle, which is less efficient in terms of gas usage but ensures a consistent supply. Continuous flow is the standard for sleep, high oxygen demand, and situations where breathing patterns are irregular or unpredictable.
Pulse dose (also called demand delivery) uses a sensor to detect the start of each inhalation and delivers a precisely timed burst of oxygen only at that moment. Because oxygen is not wasted during exhalation, pulse dose units feature longer battery life and are lighter than continuous flow devices of equivalent output. This makes pulse dose the preferred choice for active daytime users who need a device they can carry comfortably.
Key differences at a glance:
- Continuous flow suits sleep, exercise with high demand, and patients with irregular breathing patterns
- Pulse dose suits active daytime use, travel, and patients with stable, detectable inhalation effort
- Pulse dose devices are lighter and have longer battery life due to on-demand delivery
- Continuous flow portable concentrators are heavier because they must produce oxygen constantly
- Neither method is universally superior. The right choice depends on your prescription and lifestyle
One critical point that many people overlook: pulse dose settings do not convert directly to continuous flow litres per minute. They are entirely different measurement systems, and attempting to substitute one for the other can result in inadequate oxygen delivery. Your prescription will specify the exact mode and setting. Never adjust this without clinical guidance.
Pro Tip: If you use a pulse dose device during the day, your clinician may still prescribe a continuous flow device for overnight use. Nocturnal oxygenation requirements differ from daytime needs, and pulse dose devices can miss breath triggers during deep sleep.
What are the oxygen delivery interfaces and when is each used?
The interface is the physical connection between the oxygen supply and your airway. Interfaces range from nasal cannula through various masks to paediatric tents, and the choice directly affects how much oxygen you actually receive.
Common oxygen delivery interfaces support different flow rates from 1 to 15 L/min depending on device type and clinical need:
| Interface | Flow rate range | Approximate FiO₂ | Typical use case |
|---|---|---|---|
| Nasal cannula | 1–6 L/min | 24–44% | Mild hypoxia, long-term home use |
| Simple face mask | 5–10 L/min | 35–55% | Moderate oxygen need, short-term |
| Venturi mask | 4–12 L/min | 24–60% (precise) | COPD, where exact FiO₂ matters |
| Non-rebreather mask | 10–15 L/min | Up to 90% | Acute respiratory failure, emergency |
| Paediatric oxygen tent | Variable | Controlled environment | Children requiring humidified oxygen |
The nasal cannula is the most widely used interface for home oxygen therapy. Two small prongs sit just inside the nostrils, leaving the mouth free for eating and speaking. It is comfortable for extended wear and suits mild to moderate oxygen needs, including most COPD management programmes.
The Venturi mask is particularly important for oxygen therapy for COPD because it delivers a precisely controlled fraction of inspired oxygen (FiO₂). COPD patients can be sensitive to excessive oxygen, which may suppress their hypoxic respiratory drive. The Venturi mask’s colour-coded diluter valves allow clinicians to prescribe exact concentrations, making it the interface of choice when precision matters more than convenience.
The non-rebreather mask is reserved for acute, high-demand situations. In emergency respiratory failure, device relevance shifts to higher flow capacity masks and manual ventilation devices, which differ fundamentally from low-flow home therapy devices. A non-rebreather mask is not a home therapy tool. If you find yourself needing one, you need emergency medical attention.
Delivery interface choice significantly affects therapy comfort and practicality, especially in paediatric care where tents and canopies allow children to receive humidified oxygen without wearing a mask, reducing distress and improving compliance.
How does hyperbaric oxygen therapy differ from standard oxygen therapy?
Hyperbaric oxygen therapy (HBOT) is a fundamentally different modality from all standard oxygen therapy types. Where conventional therapy increases the oxygen concentration you breathe at normal atmospheric pressure, HBOT increases both the oxygen concentration and the surrounding pressure simultaneously.
HBOT delivers 100% oxygen at chamber pressures of 1.5 to 2.5 atmospheres inside a pressurised chamber. At these pressures, oxygen dissolves directly into blood plasma rather than relying solely on haemoglobin transport. This dramatically increases the amount of oxygen reaching tissues, including areas with compromised circulation.
FDA-approved indications for HBOT include:
- Diabetic foot ulcers and non-healing wounds
- Carbon monoxide poisoning
- Decompression sickness (the bends)
- Radiation tissue damage (radionecrosis)
- Severe anaemia where transfusion is not possible
- Certain serious infections, including necrotising fasciitis
HBOT sessions typically last 60 to 90 minutes and are conducted in a clinical or specialist wellness setting. A course of treatment often involves multiple sessions over several weeks, depending on the indication. This is a far more structured protocol than home oxygen therapy, which may simply involve wearing a nasal cannula for a prescribed number of hours per day.
HBOT is not a substitute for standard oxygen therapy in COPD or routine respiratory conditions. It is a specialist treatment with specific indications, protocols, and safety requirements. Understanding this distinction protects you from misinformation and helps you seek the right care.
HBOT is fundamentally different because it increases pressure in addition to oxygen concentration, requiring special protocols and yielding therapeutic gains beyond what standard oxygen can achieve. For those curious about its wellness and anti-ageing applications, the hyperbaric oxygen anti-ageing benefits are increasingly well-documented and worth exploring separately.
How to choose the right type of oxygen therapy for your needs
Choosing the right oxygen therapy type is not a decision you make alone. It requires a clinical assessment, a formal prescription, and an honest conversation about your lifestyle. That said, understanding the decision-making framework helps you ask better questions and advocate for yourself.
- Establish your clinical oxygen need. Your clinician will measure your blood oxygen saturation (SpO₂) at rest, during exercise, and during sleep. The results determine your prescribed flow rate and whether continuous flow or pulse dose is appropriate.
- Consider your mobility requirements. If you are active and travel regularly, a portable pulse dose concentrator is likely your best daytime option. If you are largely home-based, a stationary concentrator offers unlimited supply without refilling.
- Address sleep separately. Device choice depends on oxygen need, mobility, and clinical context including sleep requirements. Many people need continuous flow overnight even if pulse dose covers them during the day.
- Match the interface to your comfort and condition. If you have COPD, a Venturi mask or nasal cannula at the prescribed flow rate is standard. If you need high-flow oxygen acutely, your clinical team will select the appropriate mask.
- Never self-adjust settings or switch delivery modes. Pulse dose and continuous flow settings are not interchangeable. Misuse can result in under-oxygenation without any obvious warning signs.
Pro Tip: Ask your oxygen supplier for a demonstration of your device before you leave the clinic or pharmacy. Understanding how to fit the interface correctly, check the flow rate, and troubleshoot basic issues will give you confidence and improve your therapy outcomes from day one.
Therapy type depends largely on clinical oxygen need and treatment setting, influencing both device choice and your quality of life. The right match between system, method, and interface is what turns oxygen therapy from a burden into a tool that genuinely supports your health.
Key takeaways
Oxygen therapy is not a single treatment. It is a category of therapies that differ by delivery system, delivery method, interface, and clinical purpose, and matching the right combination to your needs determines how well it works.
| Point | Details |
|---|---|
| Three core delivery systems | Compressed gas, liquid oxygen, and concentrators differ in storage, portability, and running costs. |
| Continuous flow vs pulse dose | Pulse dose is lighter with longer battery life; continuous flow is required for sleep and high oxygen demand. |
| Interface determines FiO₂ | Nasal cannula suits mild hypoxia; Venturi masks provide precise concentrations for COPD; non-rebreather masks are for emergencies only. |
| HBOT is a separate modality | Hyperbaric therapy operates at 1.5 to 2.5 atmospheres and has distinct FDA-approved indications beyond standard oxygen use. |
| Prescription is non-negotiable | Settings, modes, and interfaces are clinically prescribed and must not be self-adjusted or converted between systems. |
Why getting your oxygen therapy type right matters more than most people realise
From my experience working with people across a range of health and wellness contexts, the single biggest mistake I see is treating oxygen therapy as a monolithic concept. Someone hears “oxygen therapy” and assumes all devices and methods are broadly equivalent, just different shapes of the same thing. They are not.
I have spoken with people who switched from a continuous flow device to a pulse dose unit without clinical guidance, assuming the settings were comparable. They were not receiving adequate oxygen for weeks before anyone noticed. The pulse dose conversion risk is real, and it is underappreciated outside clinical circles.
What gives me genuine optimism is how rapidly portable concentrator technology has advanced. Devices that were bulky and noisy five years ago are now genuinely discreet and travel-friendly. This matters enormously for quality of life, particularly for younger patients and those managing conditions like COPD who want to remain active. If you were prescribed oxygen therapy several years ago and have not reviewed your equipment recently, it is worth asking whether newer options suit your lifestyle better.
On HBOT specifically: I think the wellness conversation around it is moving in a positive direction, but it needs to stay grounded. HBOT at a reputable facility, with proper protocols, offers real therapeutic potential. The common misconceptions about hyperbaric therapy are worth reading before you commit to a course of treatment, so you go in with accurate expectations. The therapy works. The hype sometimes oversells it.
My core advice is simple: work with your clinical team, understand your device, and do not assume that what works for someone else will work for you. Oxygen therapy is personal.
— Mark
Discover oxygen therapy and wellness support at Live5dhealth
At Live5dhealth, we believe that access to the right therapeutic tools should feel empowering, not overwhelming. Our wellness centre in Boyle, County Roscommon, offers hyperbaric oxygen therapy sessions in a supportive, professionally managed environment, alongside a full range of spa, gym, and retreat services designed to help you feel your best.
Whether you are exploring HBOT for recovery, cellular regeneration, or general vitality, our team is here to guide you through your options with clarity and care. We also stock world-class health supplements through our online wellness shop to support your health goals between sessions. For those interested in combining therapies, our guide on the vibro plate and HBOT combination explores how pairing modalities can amplify your results. Your best self is within reach. Come and find it with us.
FAQ
What is the main difference between oxygen therapy types?
The main difference lies in the delivery system, delivery method, and interface used. Compressed gas cylinders, liquid oxygen, and concentrators store and supply oxygen differently, while continuous flow and pulse dose methods determine when oxygen is delivered during the breath cycle.
Is pulse dose oxygen therapy safe for overnight use?
Pulse dose delivery is generally not recommended for overnight use because the sensor may fail to detect breath triggers during deep sleep. Continuous flow is the standard prescription for nocturnal oxygen therapy.
How does oxygen therapy for COPD differ from general oxygen use?
Oxygen therapy for COPD often requires precise oxygen concentrations to avoid suppressing the hypoxic respiratory drive. Venturi masks are commonly used because they deliver exact, controlled FiO₂ values, unlike standard nasal cannulas which provide variable concentrations.
Can I use hyperbaric oxygen therapy at home?
Clinical-grade HBOT at 1.5 to 2.5 atmospheres requires a pressurised chamber and professional supervision. Mild hyperbaric chambers for home use operate at much lower pressures and are not equivalent to medically approved HBOT protocols.
How do I know which type of oxygen therapy is right for me?
A clinician will assess your blood oxygen saturation at rest, during activity, and during sleep to determine your flow rate, delivery mode, and interface. Never self-prescribe or adjust oxygen settings without medical guidance.